Chronic Hepatitis
W. Ali H. MD Medicine (I), Tina M. St. John, MD

Overview: Chronic Hepatitis
Hepatitis is the Latin term for liver inflammation.
It is characterized by hepato-necrosis and inflammatory cell infiltration.
Viral and toxic agents are the most common causes of hepatitis. Acute hepatitis describes a process enduring less than 6 months.
Hepatitis is deemed chronic when it is present for longer than 6 months.
The ongoing inflammatory process may lead to fibrosis and eventually cirrhosis, with a concomitant increased risk of hepato-cellular carcinoma.
Chronic hepatitis has various causes, in isolation or combination.
Most people with chronic hepatitis develop the disease gradually without an acute clinical illness or obvious symptoms.
The condition is generally insidious and slowly progressive, declaring itself clinically only after cirrhosis develops with concomitant symptoms.
Cases of chronic hepatitis diagnosed before the development of hepatic symptoms are often the result of incidental findings, especially unexpectedly elevated liver enzymes on routine biochemical panels.
Liver biopsy remains the gold standard for making a histo- pathologic diagnosis of chronic hepatitis.
Biochemical, serologic, and nucleic acid testing are the mainstays of etiologic diagnosis.
Histologic information is particularly important for hepatitis C management decisions because fibrotic stage is often a key factor in such deliberations.
Overall, approximately 5% to 25% of people with CHC develop cirrhosis over a period of 25 to 30 years.
Observational prospective studies and outcome modeling projections indicate that the risk of liver disease progression toward severe fibrosis or cirrhosis is minimal at 10 to 15 years in patients with persistently normal alanine amino-transferase (ALT) levels.
Approximately 5% to 10% in patients with elevated ALT and no fibrosis on initial liver biopsy, but greater than 30% to 40% in those with elevated ALT and portal fibrosis.
Important Points to Consider
Nonhistologic Factors Associated With Increased Risk of Development of Cirrhosis Among People With Chronic Hepatitis C
Genotypic male
Heavy alcohol consumption
Coinfection with human immunodeficiency virus and/or hepatitis B virus
Elevated serum alanine aminotransferase
Obesity
Age older than 35 yr at the time of initial infection
Other Points
Patients with chronic hepatitis should be vaccinated against hepatitis A and B to decrease the risk of superinfection and acute fulminant hepatitis.
A challenge in pharmaceutical treatment is that patients who are most likely to respond to therapy are also least likely to progress to cirrhosis.
Patients with chronic hepatitis should be vaccinated against hepatitis A and B to decrease the risk of superinfection and acute fulminant hepatitis.
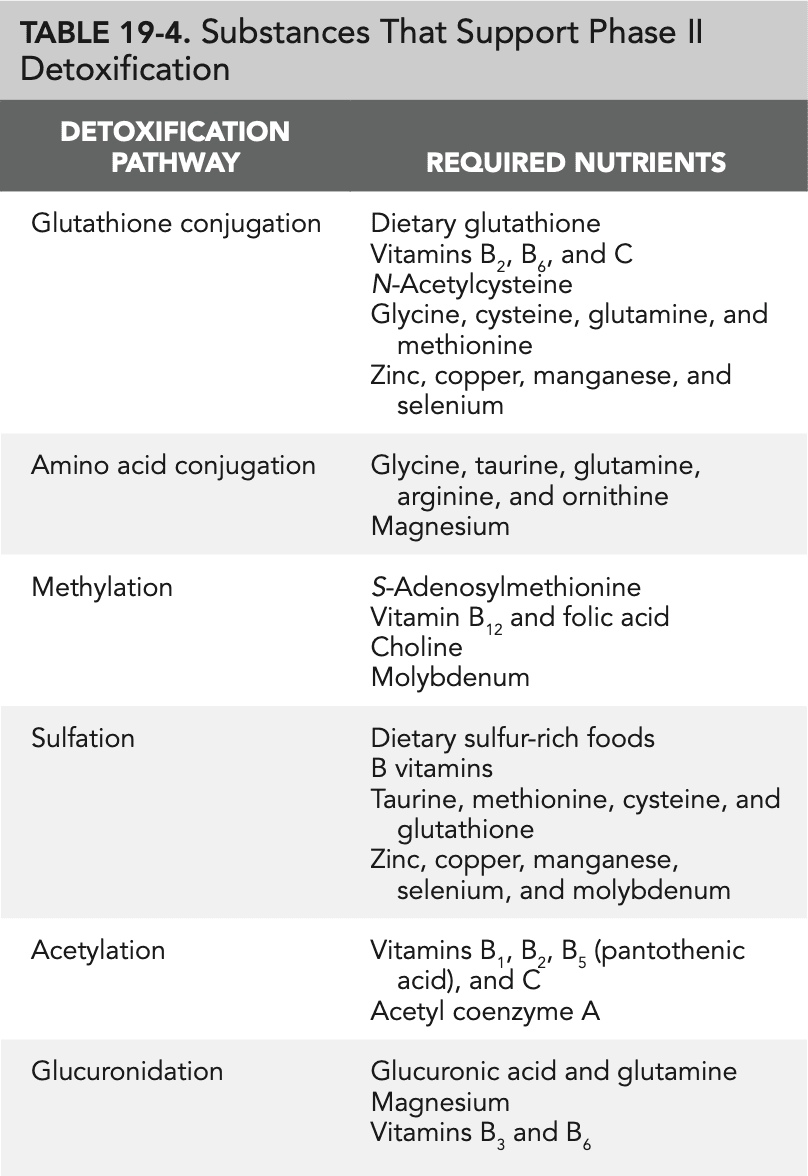
Glutathione is not absorbed well when taken orally.
The best way to increase glutathione levels is to eat sulfur-containing foods (asparagus, avocados, broccoli, spinach, garlic) and supplement with nutrients that enhance production, including vitamin C, vitamin E, N-acetylcysteine, selenium, silymarin, and curcumin.
Hepatitis C genotypes 1 and 4 are associated with the poorest response to therapy.
Steatohepatitis is more common with genotype 3 disease and is associated with a lower response rate to interferon- based therapy. Management of metabolic syndrome, high triglycerides, and obesity should be a priority.
Substances That Support Phase II Detoxification
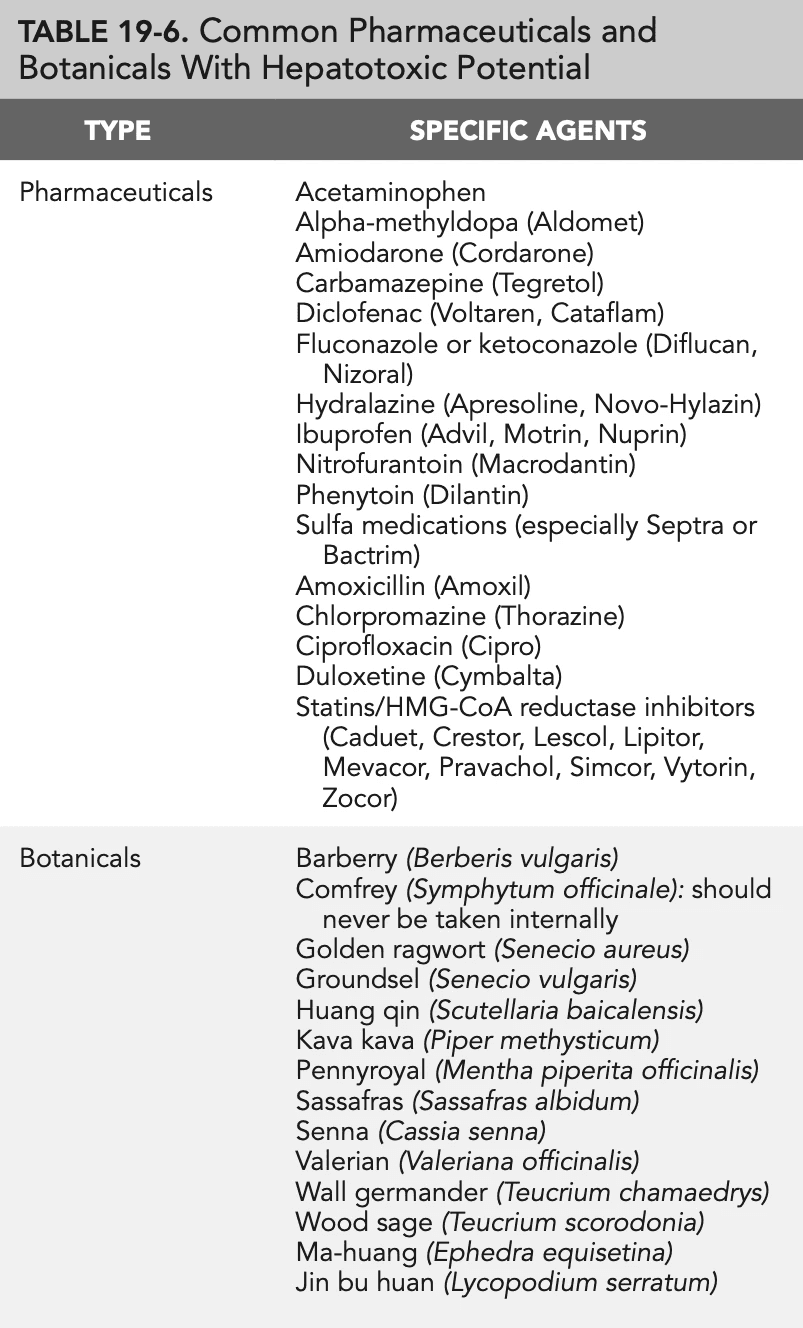
Common Pharmaceuticals and Botanicals With Hepatotoxic Potential
Prevention Prescription: Chronic Hepatitis
Hepatitis B Primary Prevention
Administer the hepatitis B vaccine.
Use universal body fluid precautions.
Hepatitis C Primary Prevention
Injection drug users: do not share needles or other drug paraphernalia.
Do not share personal care items that may be contaminated with blood, including toothbrushes, razors, and manicure and pedicure equipment.
Do not get a tattoo with an unsterilized stylus; be certain that new ink and new or sterilized ink pots are used.
If you have multiple sexual partners, avoid contact with blood during sexual activity, and use latex condoms correctly and consistently at every sexual encounter.
Use universal body fluid precautions.
Hepatitis C Secondary Prevention
Abstain from alcohol.
Abstain from tobacco products, street drugs, and unnecessary medications and supplements.
Avoid environmental toxins, including pesticides, herbicides, and other toxic chemicals.
Achieve and maintain a healthy body weight.
Exercise regularly.
Establish and maintain on going healthcare to include monitoring for disease progression and screening for the development of hepatocellular carcinoma.
Therapeutic Review: Chronic Hepatitis
Screening
Because people with chronic hepatitis C (CHC) are likely to be asymptomatic and may not have consistently elevated liver enzymes, all patients should be routinely screened for hepatitis C risk factors. The following list of questions can help elucidate a patient’s relative risk for hepatitis C:
Did you receive any blood or blood products (e.g., packed cells, whole blood, plasma, platelets, clotting factors, gammaglobulin) before 1992?
Have you ever undergone kidney dialysis?
Have you had an organ transplant (especially before 1992)?
Have you ever, even once, injected street drugs?
Have you ever, even once, shared drug paraphernalia (e.g., needles, cookers, straws)?
Have you ever been accidentally stuck with a used medical needle?
Do you have human immunodeficiency virus (HIV)?
Have you ever held a job (e.g., police officer, firefighter, emergency medical technician, paramedic, medical or dental worker) or participated in a sport (e.g., hockey, rugby, boxing, football, and other contact sports) that exposed you to blood?
Did your mother have hepatitis C when you were born?
Have you ever been incarcerated?
Have you been in military combat?
Are you living with or have you ever lived with someone known to have hepatitis C?
Have you ever shared personal care items that may have been contaminated with blood (e.g., razors, toothbrushes, manicure or pedicure equipment) with others?
Have you ever had a piercing or tattoo in a noncommercial facility?
Have you ever had unprotected sex with someone known to have hepatitis C?
Have you ever had unprotected sex with someone who is or was an injection drug user?
Sexual Transmission
Sexual transmission of hepatitis C is uncommon, especially among people in a long-term, monogamous relationship. However, patients with a history of sexually transmitted infections and multiple, short-term sexual relationships are at increased risk. Sexual behavior that involves contact with blood is the source of potential hepatitis C virus (HCV) exposure (e.g., anal intercourse, fisting, and other practices that can cause bleeding).
Laboratory Testing
Patients with one or more risk factors and those patients who specifically request testing should be screened for hepatitis C by using an enzyme immunoassay for HCV antibodies.
A positive serologic test result indicates exposure to the virus but not necessarily active infection.
Approximately 25% to 35% of adults infected with HCV spontaneously clear the virus.
The remaining 65% to 75% become chronically infected.
Patients with a positive antibody screen should be tested for HCV RNA to determine whether they are currently infected.
HCV genotype testing is recommended for any patient considering interferon-based therapy because genotype affects the planned duration of treatment and the probability of successful viral clearance.
Although liver biopsy was once considered a standard component of the initial evaluation of patients with CHC, the American Association for the Study of Liver Diseases now recommends that physicians consider obtaining a liver biopsy only if the patient or provider believes that the information will contribute to therapeutic decision-making or will provide desired prognostic information.
For patients who prefer not to undergo a liver biopsy or who have a contraindication to the procedure, panels of serum markers for fibrosis (e.g., Fibrotest, Fibrosure) may help evaluate the liver at risk. These tests are reasonably accurate at differentiating the extremes of the fibrotic spectrum (i.e., little to no fibrosis vs. cirrhosis). The ability to determine the degree of fibrosis between the extremes of the spectrum is limited.
The following therapeutic review addresses management after a diagnosis of CHC has been made and liver histologic features have been evaluated, directly or indirectly
Patients With Newly Diagnosed CHC Who Have No Physical, Laboratory, or Histologic Evidence of Advanced Fibrosis or Cirrhosis and Who Are Not Undergoing Interferon-Based Therapy
Laboratory
Obtain baseline markers of liver status (aspartate aminotransferase [AST], alanine aminotransferase [ALT], albumin, bilirubin, and platelet count) and alfa-fetoprotein level.
Consider HCV genotype testing to aid in management decisions.
Monitor the AST/ALT ratio at least biannually.
Radiology
Obtain a baseline ultrasound study of the liver.
Lifestyle
Reduce toxin exposure (e.g., tobacco, environmental toxins).
Urge abstention from alcohol and illicit drug use.
Reduce dietary toxins; encourage organic foodstuffs if feasible.
Encourage achieving and maintaining a healthy body weight.
Promote regular exercise.
Counsel patients about how to reduce the risk of spread of chronic viral hepatitis to others.
Refer for alcohol or drug dependence counseling and treatment as needed.
Nutrition
Fruits and vegetables
Increase intake of fruits and vegetables (especially cruciferous vegetables) to six or seven servings daily.
Limit grapefruit and other inhibitors of the detoxification system.
Dietary fats
Limit fat intake (no more than 30%; aim for 10% to 20%).
Eliminate trans fats (hydrogenated and partially hydrogenated oils).
Use olive, canola, or peanut oil in cooking.
Increase intake of omega-3 fatty acids (cold-water fish, nuts, flaxseed).
Decrease intake of omega-6 fatty acids (vegetable oils).
Dietary fiber
Increase fiber intake.
Consider supplementation with methylcellulose or psyllium if dietary fiber intake is inadequate.
Dietary protein
Ensure adequate protein intake (recommended grams of intake = pounds of body weight × 0.5 to 0.7).
Pharmaceuticals
Vaccinate patients without immunity to hepatitis A and B.
Mind-Body Therapy
Encourage lifestyle choices that reduce psychosocial stress.
Explore relaxation and meditative techniques tailored to the patient’s personality, belief system, and culture to help reduce stress.
Supplements
Selenium: 200 mcg daily
Iron-free multivitamin with minerals: daily
B-complex vitamin: daily
Vitamin C: 200 to 250 mg twice daily
Vitamin E (d-alpha tocopherol): 400 units daily
Precautions: Avoid iron supplementation and excess vitamin A.
Botanicals to Consider
Silymarin phosphatidylcholine: 240 mg twice daily
Licorice root: 200 to 500 mg dry powder three times daily or 1 to 2 g powdered root three times daily or 2 to 4 mL of fluid extract three times daily
Schisandra: 100 mg of extract twice daily
Astragalus: 4 to 7 g of powder daily
Monitoring
See the patient at least twice yearly to monitor for signs of progression or extrahepatic manifestations of disease.
Monitor the AST/ALT ratio; a ratio greater than 1 indicates probable disease progression to advanced fibrosis or cirrhosis. Refer for a gastroenterology or hepatology consultation.
Consider repeat liver biopsy every 4 to 5 years.
Consultations
An infectious disease consultation and comanagement are highly recommended for patients coinfected with HCV and HIV.
A gastroenterology or hepatology consultation is recommended for patients coinfected with HCV and HBV and for patients with HCV and other comorbid hepatic conditions.
Patients With Newly Diagnosed CHC Who Have Physical, Laboratory, or Histologic Evidence of Advanced Fibrosis or Cirrhosis
Recommendations are the same as previously described, with the following additions:
Laboratory
Order HCV genotype testing to aid in treatment planning.
Order baseline HCV viral load to aid in treatment planning.
Lifestyle
Same as previously described.
Nutrition
A nutrition consultation is recommended for patients with cirrhosis.
Mind-Body Therapy
Same as previously described.
Pharmaceuticals
Recommend peginterferon alfa plus ribavirin treatment for patients without contraindications to this therapy (Table 19-7).
For patients with relative contraindications, prepare and execute a management plan to resolve the contraindications.
Monitoring Patients Receiving Peginterferon plus Ribavirin
Office visits
Monitor patients who are receiving therapy at least every 4 weeks for treatment side effects, including depression.
Treat side effects aggressively to improve compliance, minimize discomfort, and avoid dose reductions. Encourage patients to call between visits if problems arise.
Laboratory testing
Monitor hemoglobin levels monthly for evidence of hemolytic anemia secondary to ribavirin.
Consider determining the HCV viral load at week 4 of treatment to determine whether the patient has had a rapid virologic response (RVR). This information may help determine the minimum duration of therapy if the patient has difficulty tolerating the planned course of treatment.
Obtain an HCV viral load measurement at week 12 of treatment to determine whether an early virologic response (EVR) has occurred. In patients without at least a 100-fold drop in HCV viral load (compared with baseline), discontinue therapy. For genotype 1 disease with EVR, continue therapy for a total of 48 weeks. For genotype 2 or 3 disease with EVR, continue therapy for a total of 24 weeks.
Check the HCV viral load at the completion of a full course of therapy to determine end-of-treatment response. Patients with detectable HCV RNA at the end of treatment are deemed nonresponders. Those without detectable HCV RNA at the end of treatment are viral responders.
End-of-treatment responders should have an HCV RNA test every 6 months for the first year and yearly thereafter for 5 years to detect possible relapse.
Botanicals
Because the potential interactions among peginterferon, ribavirin, and botanicals have not been evaluated, consider discontinuing all herbal supplements during interferon-based therapy or monitor the patient closely for new or unexpected symptoms or reactions.
Consultations
A nutrition consultation is recommended for patients with cirrhosis.
If botanicals are to be continued during interferon-based therapy, consider consulting with a Chinese medicine specialist experienced in the management of patients with CHC who are receiving interferon-based therapy.
An infectious disease consultation and comanagement are highly recommended for patients coinfected with HCV and HIV.
A gastroenterology or hepatology consultation is recommended for patients coinfected with HCV and HBV and for patients with HCV and other comorbid hepatic conditions.
For patients with compensated cirrhosis, a hepatology consultation is strongly recommended before treatment. Interferon-based therapy can push patients with compensated cirrhosis into decompensation.
Patients With Newly Diagnosed CHC and Moderate Fibrosis to Compensated Cirrhosis Who Have Contraindications to or Decline Interferon-Based Therapy
Management of these patients is generally the same as for patients with minimal fibrosis, with a few exceptions. Monitor carefully with periodic biochemical testing (AST, ALT, total protein, albumin, bilirubin, white blood cell count, and platelet count).
Monitor for development of hepatocellular carcinoma with alfa-fetoprotein testing every 6 months and hepatic ultrasound at least once yearly. Botanical therapy may be advised in these patients.
Additional supplements (not previously mentioned in the recommendations for patients with minimal fibrosis) should be considered to reduce hepatic inflammation, boost hepatic antioxidant capacity, promote robust immune function, and support the detoxification pathway (i.e., glutamine, alpha-lipoic acid, N-acetylcysteine, and S-adenosylmethionine).
Patients With CHC Who Were Previously Treated Unsuccessfully With Standard Interferon plus Ribavirin (Nonresponse and Relapse)
Patients previously treated with standard interferon plus ribavirin or just with interferon who were nonresponders or who relapsed after completion of therapy can be successfully retreated with peginterferon alfa plus ribavirin. Response rates are generally not as high as in treatment-naive patients, especially among previous treatment nonresponders.
The FDA recently approved the protease inhibitors telaprevir (Incivek) and boceprevir (Victrelis), which can be added to peginterferon and ribavirin as triple therapy for patients with genotype 1 CHC. The addition of one of these protease inhibitors increases the probability of response to peginterferon and ribavirin in this difficult-to-treat population.
Patients With CHC and Decompensated Cirrhosis
Refer for a hepatology consultation and possible liver transplant evaluation.
Key Web Sources
National HIV/AIDS Clinicians’ Consultation Center. http://www.nccc.ucsf.edu/
The Body, a subsidiary of HealthCentral Network. http: //www.thebody.com/index.html
Johns Hopkins Medicine. http://hopkins-aids. edu/. http://locator.aids.gov/
National Institutes of Health HIV/AIDS Prevention & Service Provider Locator. www. aidsinfo.nih.gov
Read more