Hormone Replacement in Women
Pamela W. Smith, MD, MPH

Overview: Hormone Replacement in Women
A woman's hormonal response is as unique to her as her own fingerprints. Hormonal replacement at any age should not be considered without a thorough understanding of all the hormones in a body.
The hormones are part of a symphony, and everything needs to be playing in tune. If one hormone is not in concert, then the patient will have a difficult time achieving optimal health.
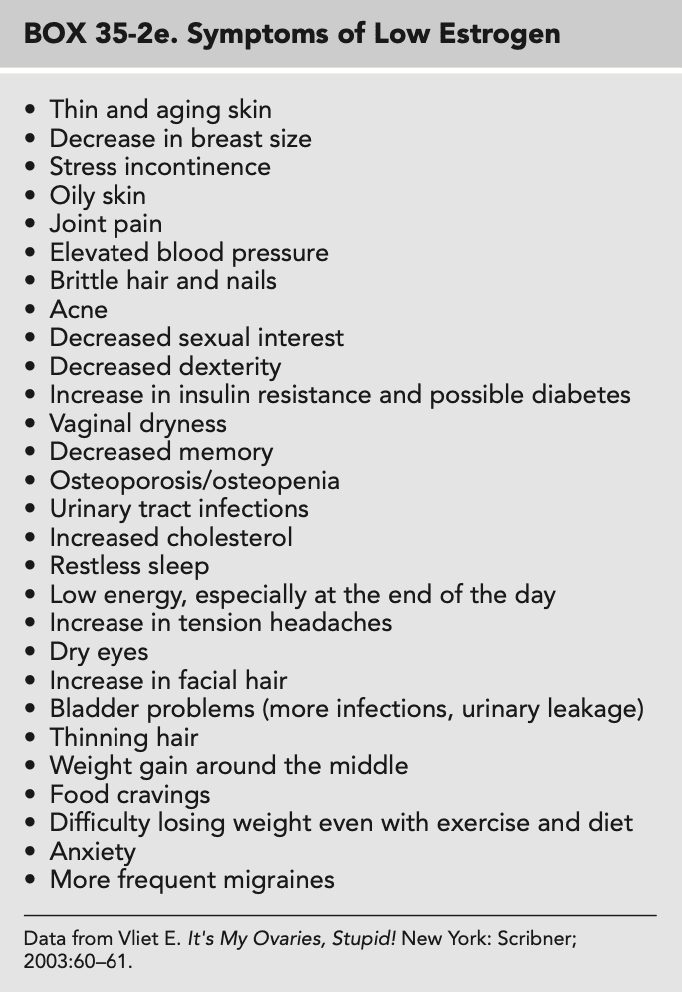
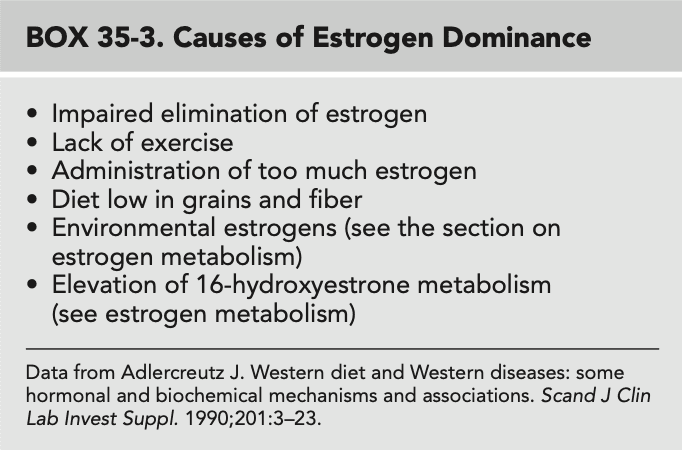
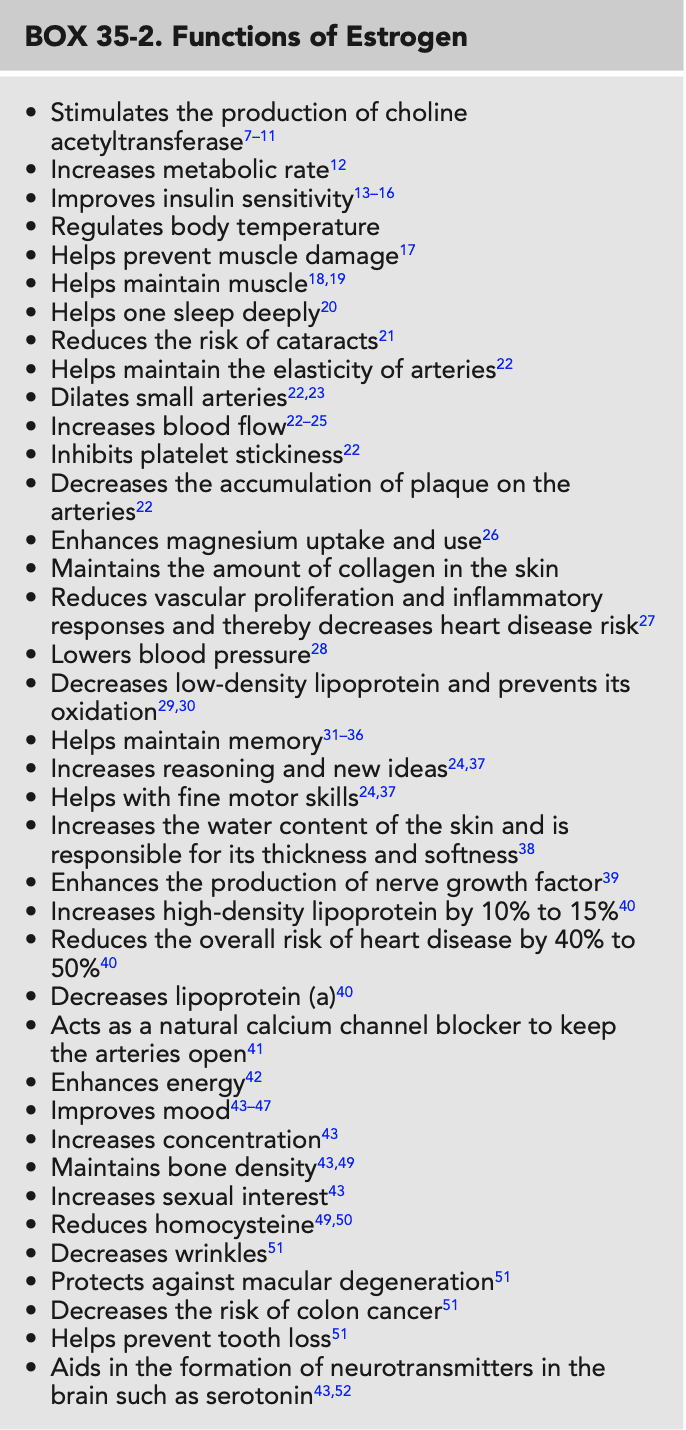
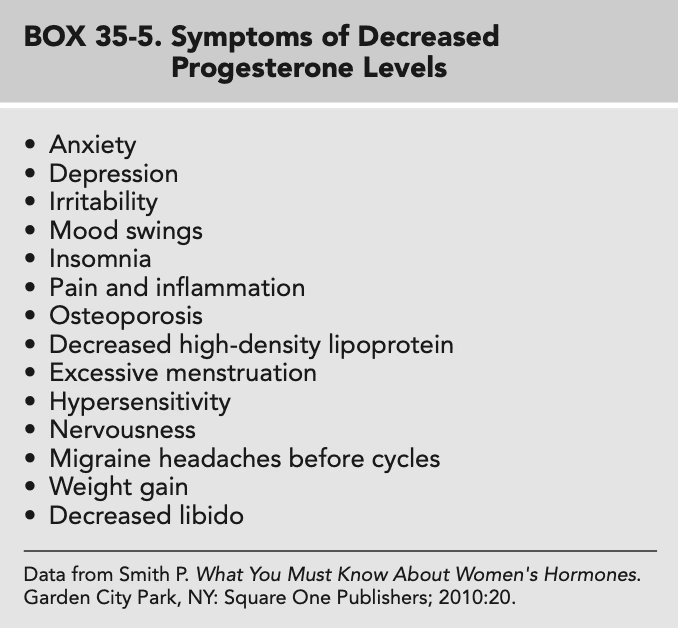
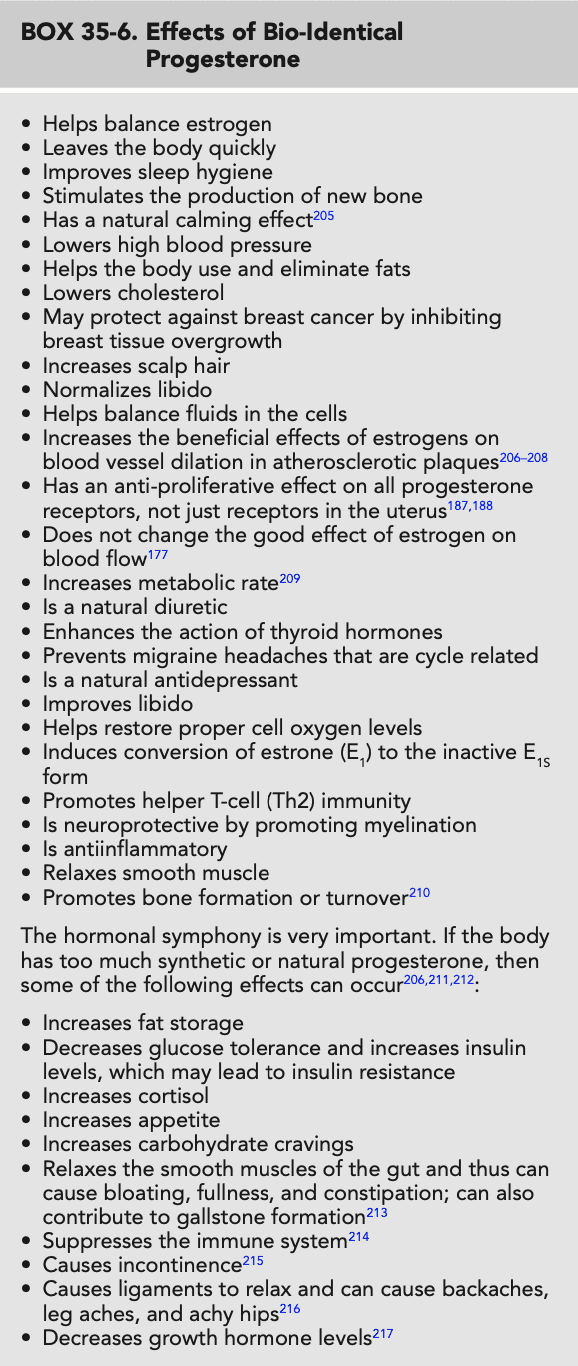
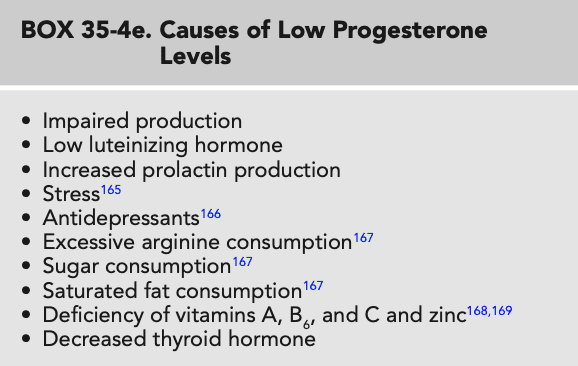
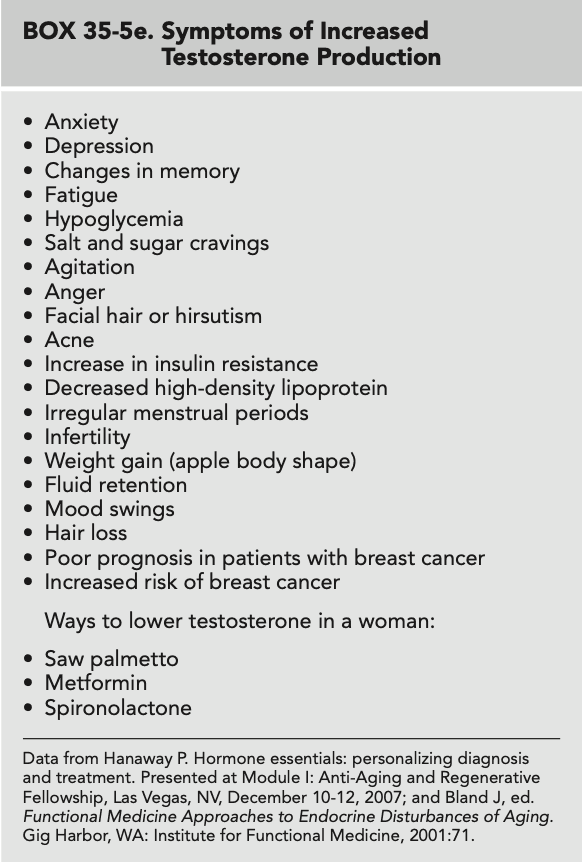
This chapter discusses the functions, symptoms of hormone deficiency, and symptoms of hormone excess with regard to estrogen, progesterone, and testosterone.
Hormone replacement of estrogen, progesterone, and testosterone is also examined. Other hormones such as dehy droepiandrosterone (DHEA), cortisol, insulin, pregnenolone, prolactin, and thyroid are also part of the hormonal web but because of space constraints are not discussed in this chapter.
Hormonal dysfunction can occur at any age. This chapter focuses on hormone replacement therapy (HRT) for women in the perimenopausal and menopausal years.
Natural Estrogens The body makes many kinds of estrogens. The three main estrogens are as follows:
E1, called estrone
E2, called estradiol
E3, called estriol
Estrone (E1)
E1 is the main estrogen the body makes post-menopausally.
It is derived from E2. High levels stimulate breast and uterine tissue, and many researchers believe it may be related to an increased risk of breast and uterine cancer.
Before menopause, E1 is made by the ovaries, adrenal glands, liver, and fat cells.
Premenopausally, E1 is converted to E2 in the ovaries.
Postmenopausally, little E1 becomes E2 because the ovaries stop working.
In later years, E1 is then made in the fat cells and, to a lesser degree, in the liver and adrenal glands.
Therefore, the more body fat one has the more E1 will be manufactured. Consequently, obese women have an increased E1:E2 ratio.60 In addition, routine alcohol consumption shifts the estrogen production to E1.
Estradiol (E2)
E2 is the strongest estrogen. It is 12 times stronger than E1 and 80 times stronger than E3.
It is the main estrogen the body produces before menopause.
Most E2 is made in the ovaries.
High levels of E2 are associated with an increased risk of breast and uterine cancer.
E2 is the main estrogen the patient loses at menopause.
However, two thirds of postmenopausal women up to the age of 80 years continue to make some E2.
E2 levels are lower in women who have had a surgical procedure that affected their ovaries.
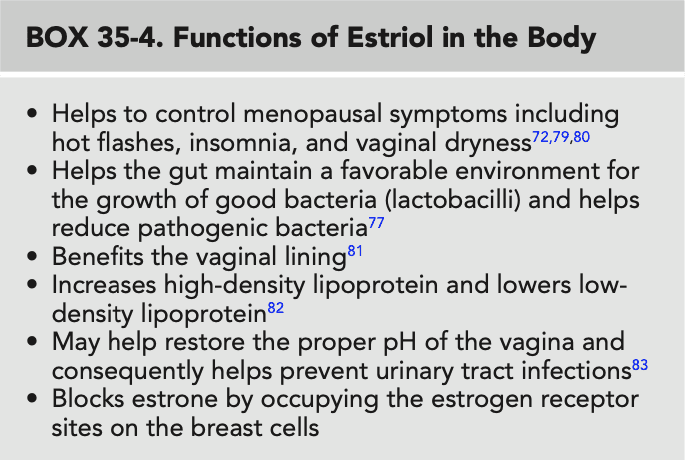
Estriol (E3)
E3 has a much less stimulating effect on the breast and uterine lining than does E1 or E2.
E3 has been shown not to promote breast cancer, and considerable evidence indicates that it protects against the disease.
In Western Europe, E3 estrogen has been used for decades.

Important Points to Consider
Obesity and alcohol increase estrone-to-estradiol ratio and may thus increase the risk of breast and uterine cancer.
Estrogen replacement therapy should be administered by the transdermal route. Oral dosing can increase the risk of heart disease, a finding that may help explain the elevated risk in the Women's Health Initiative study
Estrone (E,) selectively activates estrogen receptor sites that increase cell proliferation and has the greatest risk of stimulating breast cancer.
Progesterone must balance with estrogen in the body.
Testosterone increases plaque formation in the coronary vessels unless it is balanced with estrogen.

Prevention Prescription
The body is designed not to need HRT postmenopausally. The adrenal glands produce enough dehydroepiandrosterone (DHEA) to make sufficient estrogen and testosterone to maintain function. Similarly, pregnenolone makes adequate progesterone, estrogen, testosterone, DHEA, and cortisol to maintain function in most patients. This function can be maintained best by the following recommendations:
Encourage regular exercise. Maintain optimal weight.
Maintain an adequate sleep-wake cycle with 7 to 8 hours of uninterrupted sleep each night.
Decrease exposure to xenobiotics that can have hormonal influences by eating organic foods,
drinking filtered water, avoiding petroleum-based cosmetics, storing food in glass (not plastic).
avoiding eating animal fat, and avoiding diesel exhaust.
Make changes to avoid chronic emotional stress (see Chapter 93, Relaxation Techniques).
Eat a diet rich in protein, ground flaxseed, green tea, omega-3 fatty acids, and cruciferous vegetables. Obtain protein from plant sources (beans, nuts) more than from animal sources.
Integrative therapeutics review
Hormone replacement therapy (HRT) is all about balance and individualized treatment dosages. Needs change over time, and ongoing reevaluation is beneficial through relationship-centered care.
Laboratory
The levels of all three estrogens (along with progesterone, testosterone, dehydroepiandrosterone DHEA), cortisol, and thyroid hormones) must be measured before the patient is prescribed HRT, and regularly thereafter, to help maintain the patient on the optimal amount of each hormone.
Lifestyle
Many positive lifestyle behaviors can be protective by increasing 2-hydroxyestrone levels.
Regular moderate exercise.
Weight loss is encouraged if the patient is overweight. This is one of the most important goals in balancing hormones in overweight women.
Nutrition
Cold water fish twice weekly
Cruciferous vegetables including broccoli, cabbage, Brussels sprouts, kale, and cauliflower
Botanicals
Kudzu (rich in isoflavones): 100 mg daily
Turmeric extract: 500 to 1000mg two to three times a day
Supplements
If homocysteine is elevated, suspect poor methylation.
Supplement with the following: vitamin B, 50 mg daily, vitamin B, 1000 mcg weekly, and folic acid, 800 mcg daily to increase 2-hydroxyestrone levels.
Fish oil with eicosapentaenoic acid and docosahexaenoic acid: 1000 mg daily
Zinc if deficient: 15 to 30 mg daily (needed for testosterone metabolism)
Indole-3-carbinol 300 mg daily or diindolylmethane (DIM) 225 mg daily
Mind-Body Therapy
Chronic stress and anxiety are foundational elements in hormone imbalance because the perception of stress has a direct effect on the hypothalamic-pituitary axis (see Chapter 93, Relaxation Techniques).
Pharmaceuticals (Hormones)
A practitioner usually begins by prescribing 20% estradiol (E) and 80% estriol (E). Then the percentages of E, and E, are adjusted according to repeated laboratory testing. The combination of E_{2} and E_{1} together is called biest and is a prescription that a compounding pharmacist can formulate. Any percentage of these two estrogens can be used because the dosage is individualized. Start low and go slow.
Progesterone
For premenstrual syndrome
Consider progesterone alone cyclically
Oral administration of sustained-release capsules (compounded) or micronized progesterone (Prometrium; comes in 100- and 200-mg formulations), at 25 to 400 mg (most common, 50 to 200 mg) given cyclically from days 12 to 24 of the menstrual cycle
Topical administration, at 5 to 50 mg applied daily on days 14 to 25 of the cycle
For perimenopause
Oral administration and topical application with doses same as for premenstrual syndrome. The patient should use this cyclically alone or combined with estrogen.
Use the lowest possible dose of progesterone in patients with obesity or metabolic syndrome.
For postmenopausal or surgical menopause status
Oral sustained-release capsules (dose at bedtime because of sedation) 50 to 200 mg or topical compounded cream, at 20 to 50 mg daily. Patients may also use 100 mg of Prometrium at bedtime if this dose is needed (lowest dose available is 100 mg). Treatment may be continuous or stopped for 5 days a month.
Estrogen
For perimenopause
Bi-estrogen (80% E, 20% E_{y} ) Compound 2 mg E_{y} with 0.5 mg E_{2} per gram and start at 0.25 mg cream topically daily or twice daily, if progesterone alone does not control symptoms.
For postmenopausal status and surgical menopause
Bi-estrogen (50% E_{y} 50% E_{2} ) Compound 1 mg E_{x} with I mg E, per gram and start 0.25 mg cream topically daily or twice daily. Patients may use it continuously or stop 5 days a month.
Testosterone
For postmenopause
Topical compounded cream, at 0.25 to 2.0mg once daily
For surgical menopause
Topical compounded cream, at 0.25 to 2.0 mg daily
Converting Administration Routes
Approximate ratio for transdermal to sublingual to oral
For progesterone, estrogen, and DHEA: transdermal 1 to sublingual 2 to oral 4 to 5 For testosterone: transdermal 1 to sublingual 2 to oral 5 to 6
Other Considerations
After hormones are prescribed, the patient should have hormone levels checked again in 90 days and then every 6 to 12 months.
The evidence/harm rating for hormones is a 2. If the recommendation were equine estrogen with progestin, as used in the Women's Health Initiative study, the rating would be a 3 because of the increased risk of myocardial infarction, stroke, deep vein thrombosis, and breast cancer.
As with any therapy, hormones should be matched to the unique needs of the patient to provide the most benefit with the least amount of harm.
Key Web Sources
http://www. iacprx.org.
http://www.pccarx. com.
www.genovadiagnostics.com.
www.metametrix.com.
www.neurorelief.com.
www.zrtlab.com.
Image credits: Derek Brahney
Read more