Heartburn
W. Ali Ahmed H. MD Medicine (I), David Kiefer, MD

Overview: Gastroesophageal Reflux Disease (GERD)
Gastro-esophageal reflux disease (GERD) occurs when there is abnormal passage of acidic stomach contents, or refluxate, into the esophagus, causing symptoms or complications.
It is one of the primary causes of the informal name and symptom “heartburn,” and GERD is a common phenomenon. Estimates are that 15% to 20% of people in the United States have heartburn or regurgitation at least once a week, and 7% of people suffer from those symptoms daily.
Symptoms of GERD may include any or all of the following: retrosternal burning, acid regurgitation, nausea, vomiting, chest pain, laryngitis, cough, and dysphagia.
The injury to the esophagus can include esophagitis, stricture, the development of columnar metaplasia (Barrett esophagus), and adenocarcinoma.
A poor correlation exists between the severity of symptoms and the pathophysiologic findings in the esophagus.
For example, GERD is not the only phenomenon in the differential diagnosis of heartburn.
Many people with GERD do not have endoscopic evidence of esophagitis, and up to 40% of people with Barrett esophagus in one study did not report heartburn.
The confusing nature of this condition makes it a challenge to develop concrete screening recommendations for advanced disease.
National Health Interview Survey, based on 31,044 interviews in the United States, documented that 3.7% of people used complementary and alternative medicine for stomach or intestinal illnesses.
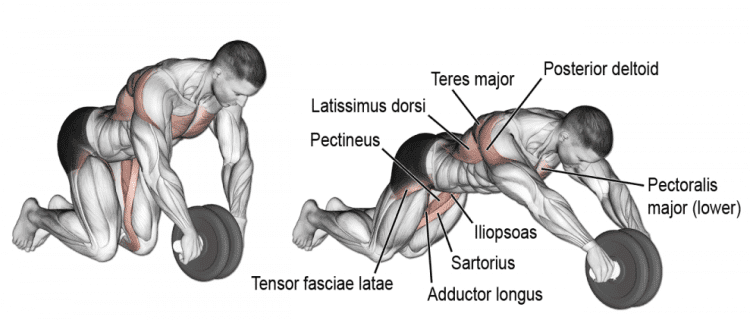
You would be surprised at the benefits received from simply using an abs-roller to strengthen your core abdominal muscles.
And also finish your meals before 7 PM.
Importants Points to Consider
Cow's milk protein is a common cause of gastroesophageal reflux disease in infants, and a trial of elimination should be considered.
The prolonged use of decoctions or infusions of dried, unprocessed licorice root can cause hypertension, hypokalemia, and edema because of the mineralocorticoid action of a saponin glycyrrhizin, also called glycyrrhizic acid.
Aggressive, long-term acid suppression can decrease the absorption of vitamin B12. Consider regular intramuscular injections of vitamin B12 for those individuals requiring long-term treatment with histamine-2 receptor blockers or proton pump inhibitors. Use of these drugs can also lead to iron malabsorption, increased risk of hip fracture, and community-acquired pneumonia.
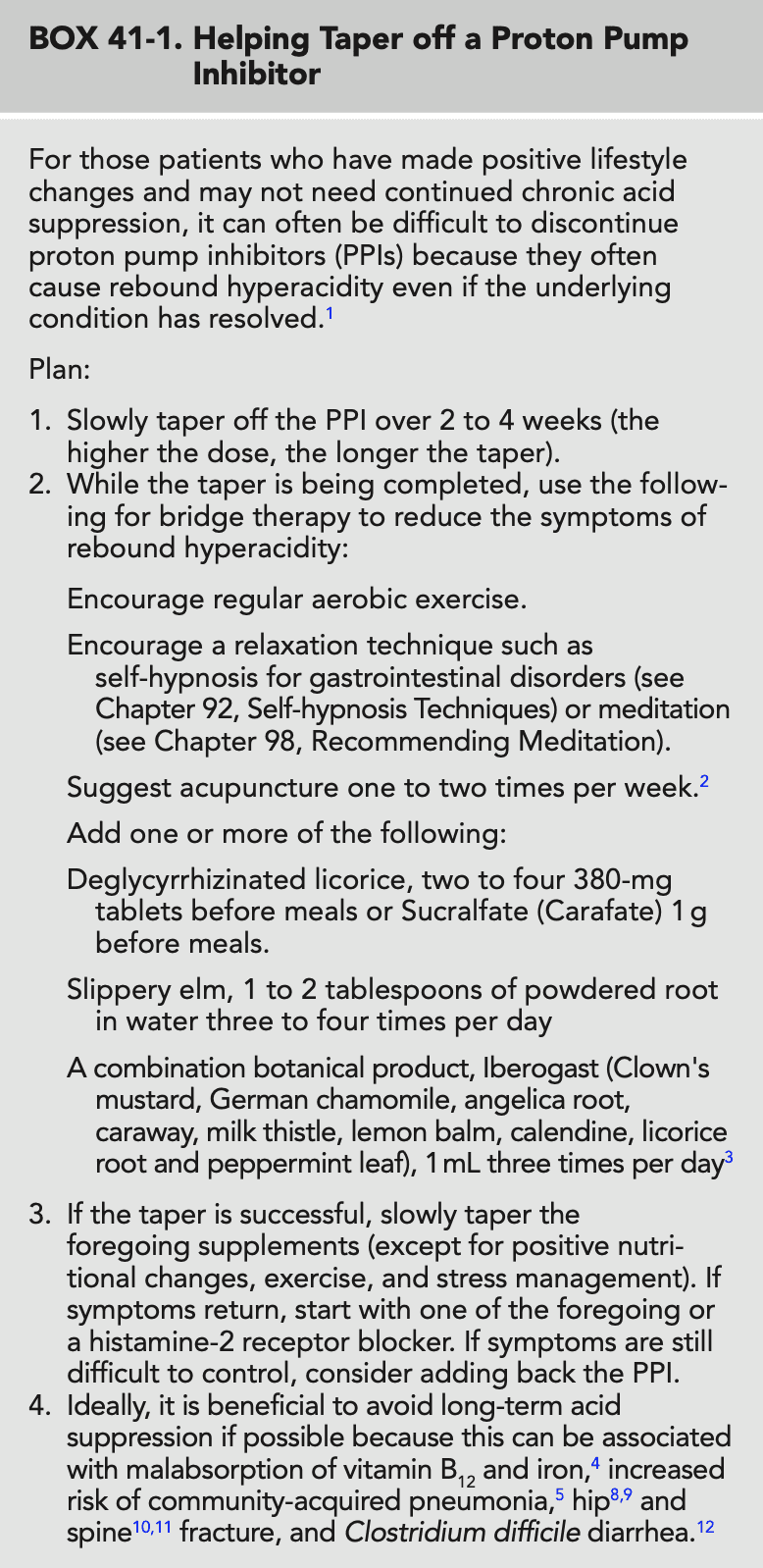
For Practitioners Trying To Help Patients Taper Proton Pump Inhibitors
Prevention Prescription
Avoid foods and supplements, and, when possible, medications known to decrease lower esophageal sphincter tone.
Ab Roller Exercises
Maintain ideal body weight. Reduce stress as much as possible, through lifestyle change and stress management and mind-body techniques.
Avoid large meals and consuming large quantities of liquids with meals.
Avoid late night meals. Take last meal 3 hours prior to sleeping.
Therapeutic Review
This summary of possible therapies is for patients with mild to moderate, short-term GERD. Patients with long-standing, more severe GERD should undergo an appropriate diagnostic workup, which may include a referral to a gastroenterologic specialist and upper endoscopy to rule out esophagitis, ulcers, Barrett esophagus, or adenocarcinoma.
Removal of Exacerbating Factors
Avoid foods, supplements, and, when possible, medications known to decrease lower esophageal sphincter tone.
If applicable, quit smoking.
If applicable, lose weight.
Lifestyle
For nocturnal symptoms, elevate the head of the bed 4 to 6 inches.
Avoid large meals and consuming large quantities of liquids with meals.
Take last meal 3 hours prior to sleeping.
Ab Roller Exercises to strengthen abdominal muscles
Mind-Body Medicine
Practice stress management and relaxation techniques.
Botanical Medicines
Deglycyrrhizinated licorice: two to four 380-mg tablets before meals
Slippery elm: 1 to 2 tablespoons of powdered root in a glass of water, three to four times daily
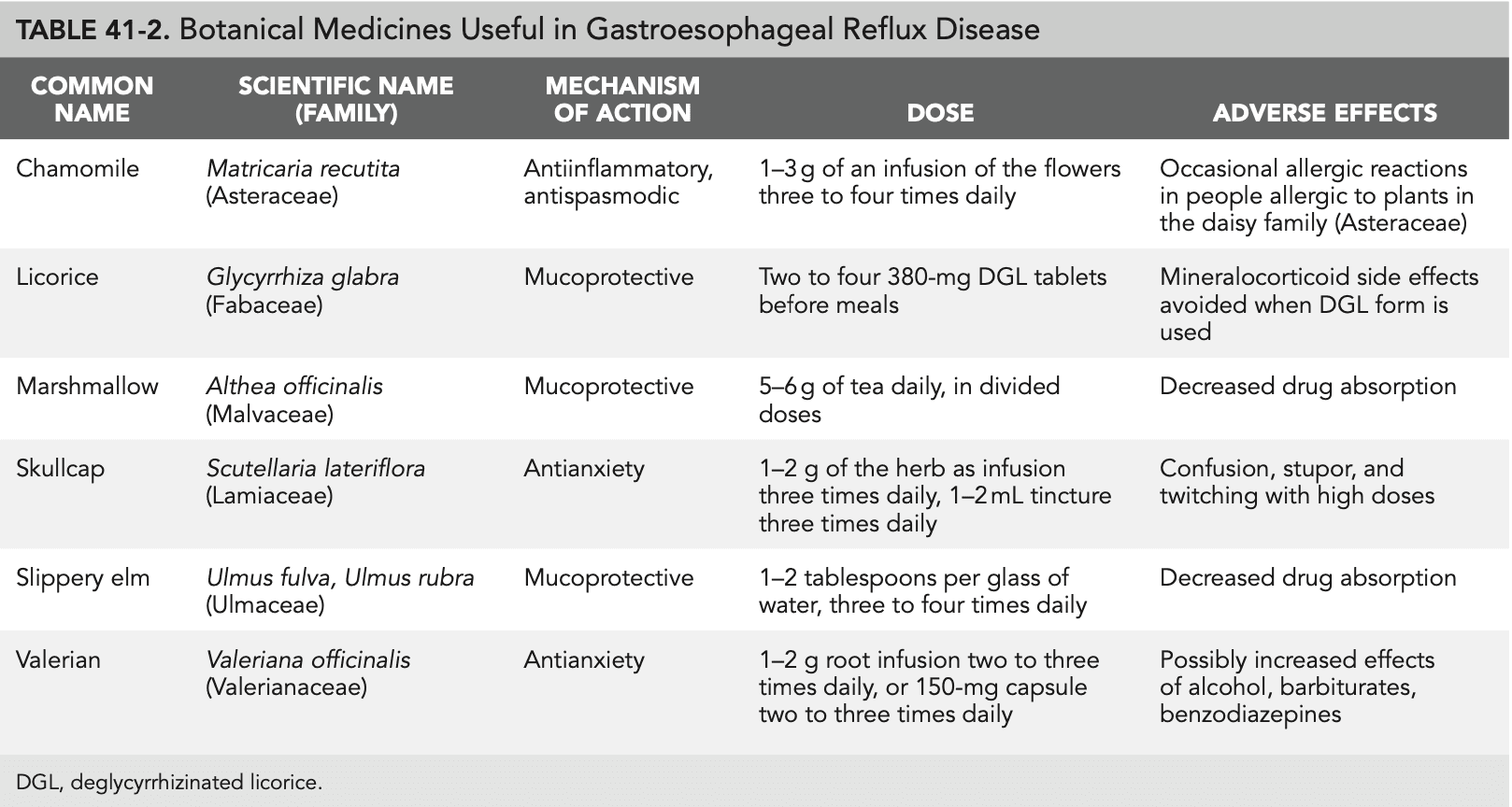
Other botanical medicines that have potential benefit include chamomile, marshmallow, skullcap, and valerian (see Table 41-2).
Pharmaceuticals
Start with a proton pump inhibitor, both for symptomatic relief and for diagnostic purposes.
Histamine-2 receptor antagonists
Over-the-counter antacids, such as calcium carbonate, aluminum hydroxide, and magnesium hydroxide, can be helpful.
Surgery
For people with intractable symptoms, fundoplication should be considered.
Key Web Sources
American College of Gastroenterology clinical updates: www.acg.gi.org/physicians/clinicalupdates.asp.
References
Goyal RK. Diseases of the esophagus. In: Kasper DL, Braunwald E, Fauci AS, et al, eds. Harrison's Principles of Internal Medicine. 16th ed. New York: McGraw-Hill; 2004.
Kahrilas PJ. Gastroesophageal reflux disease. N Engl J Med. 2008;359: 1700–1707. Wileman SM, McCann S, Grant AM, et al. Medical versus surgical management for gastro-oesophageal reflux disease (GORD) in adults. Cochrane Database Syst Rev. 2010;(3):CD003243.
Barnes P, Powel-Griner E, McFann K, Nahin RL. Complementary and Alternative Medicine Use among Adults: United States, 2002. Advance data from vital and health statistics no. 343. Hyattsville, MD: National Center for Health Statistics; 2004.
Behrman RE, Kliegman RM, Jenson HB, eds. Nelson Textbook of Pediatrics. 17th ed.Philadelphia: Saunders; 2004.
Van Deventer G, Kamemoto E, Kuznicki JT, et al. Lower esophageal sphincter pressure, acid secretion, and blood gastrin after coffee con- sumption. Dig Dis Sci. 1992;37:558–569.
Thomas FB, Steinbaugh JT, Fromkes JJ, et al. Inhibitory effect of coffee on lower esophageal sphincter pressure. Gastroenterology. 1980;79:1262–1266.
Feldman M, Barnett C. Relationships between the acidity and osmolality of popular beverages and reported postprandial heartburn. Gastroenterology. 1995;108:125–131.
Dennish GW, Castell DO. Caffeine and the lower esophageal sphincter. Am J Dig Dis. 1972;17:993–996.
Pizzorno JE, Murray ME, eds. Textbook of Natural Medicine. 2nd ed. Edinburgh: Churchill Livingstone; 1999.
MacDonald-Haile J, Bradley LA, Bailey MA, et al. Relaxation training reduces symptom reports and acid exposure in patients with gastroesophageal reflux disease. Gastroenterology. 1994;107:61–69.
Bradley LA, Richter JE, Pulliam TJ, et al. The relationship between stress and symptoms of gastroesophageal reflux: the influence of psychologi- cal factors. Am J Gastroenterol. 1993;88:11–19.
Oranu AC, Vaezi MF. Noncardiac chest pain: gastroesophageal reflux disease. Med Clin North Am. 2010;94:233–234.
Iacono G, Carroccio A, Cavataio F, et al. Gastroesophageal reflux and cow's milk allergy in infants: a prospective study. J Allergy Clin Immunol. 1996;97:822–827. 15.
Forget P, Arends JW. Cow's milk protein allergy and gastro-oesophageal reflux. Eur J Pediatr. 1985;144:298–300. 16.
Yarnell E. Naturopathic Gastroenterology. Sisters, OR: Naturopathic Medical Press; 2000. 17.
Mills S, Bone K. Principles and Practice of Phytotherapy: Modern Herbal Medicine. Edinburgh: Churchill Livingstone; 2000. 18.
Johnson LP. Pocket Guide to Herbal Medicines. Malden, MA: Blackwell Science; 2002. 19. Brinker F. Herb Contraindications and Drug Interactions. 3rd ed. Sandy, OR: Eclectic Medical Productions; 2001. 20.
van Pinxteren B, Numans ME, Bonis PA, Lau J. Short-term treatment with proton pump inhibitors, H2-receptor antagonists and prokinetics for gastro-oesophageal reflux disease–like symptoms and endoscopy nega- tive reflux disease. Cochrane Database Syst Rev. 2006;(3): CD002095. 21.
Hershcovici T, Fass R. Management of gastroesophageal reflux dis- ease that does not respond well to proton pump inhibitors. Curr Opin Gastroenterol. 2010;26:367–378. 22.
Lockie A. The Family Guide to Homeopathy. New York: Simon and Schuster; 1989. 23.
Dickman R, Schiff E, Holland A, et al. Clinical trial: acupuncture vs. doubling the proton pump inhibitor dose in refractory heartburn. Aliment Pharmacol Ther. 2007;26:1333–1344. 24.
Michelfelder AJ, Lee KC, Bading EM. Integrative medicine and gastro- intestinal disease. Prim Care. 2010;37:255–267. 25.
Broeders JA, Mauritz FA, Ahmed Ali U, et al. Systematic review and meta-analysis of laparoscopic Nissen (posterior total) versus Toupet (posterior partial) fundoplication for gastro-oesophageal reflux disease. Br J Surg. 2010;97:1318–1330. 26.
Craig WR, Hanlon-Dearman A, Sinclair C, et al. Metoclopramide, thick- ened feedings, and positioning for gastro-oesophageal reflux in children under two years. Cochrane Database Syst Rev. 2005;(2): CD003502. 27.
Werbach MR, Murray MT. Botanical Influences on Illness: A Sourcebook of Clinical Research. 2nd ed. Tarzana, CA: Third Line Press; 2000.
Read more